

INTRODUCTION
Coronavirus disease 2019 (COVID-19) is a respiratory disease caused by a novel coronavirus named severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2). Recent studies have suggested that COVID-19 positive patients present with leukopenia, lymphopenia, neutrophilia, thrombocytopenia, and higher neutrophil: lymphocyte ratio (NLR) and monocyte: lymphocyte ratio (MLR). More recently, we reported hypersegmented granulocytes and COVID-19 infection in Blood. 2020 Jun 11;135(24):2196. Neutrophil hypersegmentation has been closely associated with vitamin B12, folate and iron deficiencies, as well as methotrexate use, chemotherapy toxicity, uremia, heat stroke, myelodysplasia and Boucher-Neuhäuser Syndrome. Initially, these cytomorphologic changes may easily be overlooked or dismissed as non-specific reactive changes. In this study, we expand our initial observation on our index case to a larger case series. To the best of our knowledge, this is the largest case series to describe the concurrent lymphocyte and unique granulocyte atypia associated with SARS-CoV-2 infection.
METHODS
Study Design
2,199 patients were hospitalized in the Mount Sinai Health System from Feb 27 to April 2, 2020 with confirmed COVID-19 positivity. Data obtained for this study was covered under an Institutional Review Board (IRB) waiver, HS#:12-00133 GCO#1:12-036(0001-08)
Inclusion criteria
50 peripheral blood smears flagged for Pathologist review from March 13 - April 20, 2020 at Mount Sinai Hospital Clinical Hematology Laboratory were included in this study. All suspected COVID-19 cases were confirmed using real-time polymerase chain reaction (RT-PCR) assay to test nasal and pharyngeal swab specimens, per WHO guidelines.
Of the 50 COVID-19 positive peripheral blood smears, 39 slides were scanned and imaged with Scopio Labs X100 Full Field Digital Microscope. The X100 provided high resolution oil-immersion level images of large scanned areas. https://scopiolabs.com/hematology/
19 peripheral blood smears were blindly and independently reviewed by 4 Hematopathologists (CS, PK, JC, JTF), with particular emphasis on granulocyte cytomorphology and percent of hypersegmented neutrophils present (defined as neutrophils with 5 or more nuclear lobes in at least 3% of cells or presence of 6 or more lobes). Atypical lymphocyte morphology was also evaluated and categorized as Downey type I, II, III or plasmacytoid, while monocyte morphology was assessed for unusual nuclear folds and features. Evaluation of platelets and other abnormalities were noted. The presence and degree of significant cytologic atypia was recorded and compared to 20 COVID-19 negative blood smears.
RESULTS
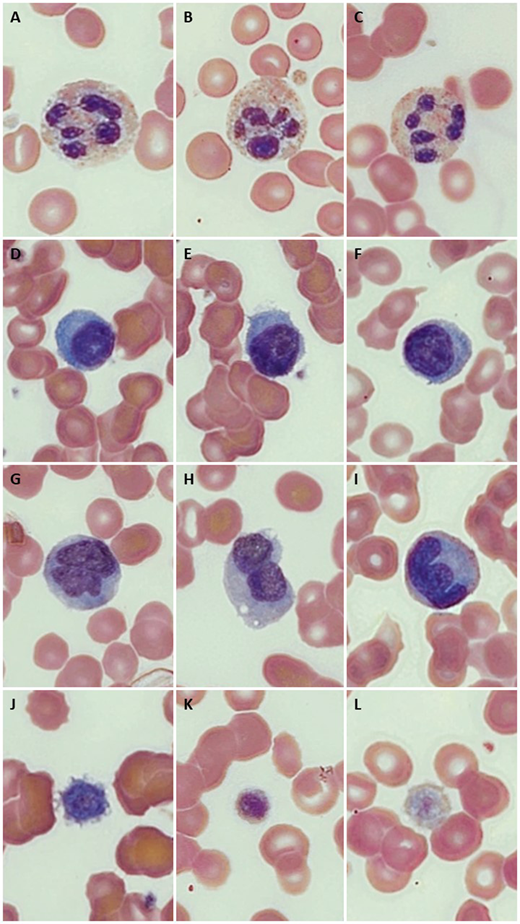
16 of the 19 (84%) COVID-19 positive cases showed hypersegmented neutrophils, and all 19 harbored atypical lymphocytes and monocyte morphology, with giant platelets. In contrast, 5 of the 20 (25%) COVID-19 negative cases showed hypersegmented neutrophils, with 2 patients displaying atypical monocytes; none showed atypical lymphocytes or giant platelets (p = 0.022). Concurrent laboratory values showed no evidence of vitamin B12 or folate deficiency. Representative images are summarized in Figure 1 (A-C, 5-6 lobed neutrophils; D-E atypical plasmacytoid lymphocytes, G-I atypical monocytes, J-L giant platelets).
CONCLUSION
We report atypical hypersegmented neutrophils with toxic cytoplasmic change, atypical monocytes, plasmacytoid lymphocytes, and giant platelets in peripheral blood smears of COVID-19 patients which are significantly higher than in control COVID-19 negative patients.
Teruya-Feldstein:Edge Anthem: Consultancy.

